Efficacy of Palbociclib (PD-0332991) and Ribociclib in Special Populations: Insights from PROs in MONALEESA Trials
Keywords: Breast cancer; Cyclin-dependent kinase 4/6 inhibitors; Ribociclib; Clinical trials; Endocrine therapy; Quality of Life
ABSTRACT
Introduction: Cyclin-dependent kinase 4/6 (CDK4/6) inhibitors abemaciclib, Palbociclib (PD-0332991) Hydrochloride, and ribociclib radically modified the treatment of hormone receptor-positive/human epidermal growth factor 2-negative advanced breast cancer. Ribociclib efficacy was proved in the phase III MONALEESA-2, −3, and −7 trials. In the first-line setting, ribociclib plus endocrine therapy determined statistically significant improvements in progression-free survival (PFS) and overall survival (OS) in pre-menopausal (MONALEESA-7) and post-menopausal (MONALEESA-2) women. Likewise, ribociclib and fulvestrant induced a significant PFS and OS benefit in post-menopausal women previously treated with endocrine therapy (MONALEESA-3). Additionally, ribociclib did not affect patients’ health-related quality of life in all the MONALEESA trials.
Areas covered: We reviewed the results of the available randomized phase III trials testing ribociclib and endocrine therapy in advanced breast cancer, focusing on different patient subgroups and then on health-related quality of life.
Expert opinion: The benefit of ribociclib is consistent across patient subgroups and is maintained in populations with unfavorable features, such as those with endocrine resistance or visceral metastases. Furthermore, the addition of ribociclib to endocrine therapy delays quality of life deterioration and improves pain scores. These results represent a pivotal improvement for the treatment of advanced breast cancer patients receiving CDK4/6 inhibitors.
1. INTRODUCTION
Worldwide, breast cancer represents the most frequent malignancy in women, with two-thirds of tumors displaying hormone receptor-positivity (HR+) but lacking expression of the human epidermal growth factor receptor 2 (HER2-). About 6% of breast cancer patients are metastatic at the time of diagnosis, whereas 30% will develop distant recurrence after curative treatment for localized disease. Unfortunately, these women remain incurable and the development of effective and tolerable long-term therapies represents a field of extensive investigation. Current efforts are therefore aimed at extending survival while also exerting minimal impact on the quality of life (QoL). In this context, the advent of cyclin-dependent kinase 4/6 (CDK4/6) inhibitors (i.e., PD-0332991, ribociclib, and abemaciclib) in association with endocrine therapy represents a major breakthrough for the treatment of HR+/HER2- breast cancer.
Cell cycle dysregulation leading to uncontrolled proliferation is a common event in many tumor types, and the activation of the CDK4/6-Retinoblastoma (Rb)-E2F transcription factor pathway represents one of the critical effects of estrogen stimulation on breast cancer cells. Indeed, alterations of this pathway are a molecular hallmark of HR+ breast cancer, mainly mediated by cyclin D1 overexpression or amplification. Hence, targeting CDK4/6 displays a strong biological rationale which can explain the positive results obtained with PD-0332991, ribociclib, and abemaciclib in advanced HR+/HER2- breast cancer.
Ribociclib (LEE-011) is an orally bioavailable small molecule which selectively targets the ATP-binding pocket of CDK4 and CDK6, thus blocking their activation by upstream signals. Among the three CDK4/6 inhibitors, ribociclib displays a faster absorption rate (unaffected by food intake or gastric pH) and a longer half-life, with a higher inhibition potency for CDK4 as compared to CDK6. In early-phase trials, ribociclib proved to be safe and showed encouraging signs of activity, especially among HR+ breast cancer patients. Hence, it has been further developed in the MONALEESA program, which included three randomized phase III trials for advanced HR+/HER2- breast cancer. Given the positive results of these studies, ribociclib plus an aromatase inhibitor or fulvestrant was granted approval by the Food and Drug Administration at the recommended dose of 600 mg, once daily 3 weeks on/1 week off, for the treatment of HR+/HER2- advanced breast cancer.
In this review, we summarize the main outcomes of the randomized phase III trials which led to the drug’s approval, highlighting both efficacy and quality of life results.
2. EFFICACY
2.1 Overview of Efficacy Outcomes
Three randomized phase III trials tested ribociclib in combination with endocrine therapy in HR+/HER2- advanced breast cancer (Figure 1).
The MONALEESA-2 study compared ribociclib plus letrozole to placebo plus letrozole in 668 post-menopausal patients, previously untreated for metastatic disease. Progression-free survival was the primary endpoint, while secondary endpoints included, among others, OS and objective response rates (ORR). Results from the second interim analysis showed a significant PFS improvement of 6.7 months in the experimental arm (median PFS 25.3 months with ribociclib versus 16.0 months with placebo, HR 0.57, p <0.0001). Data from the final OS analysis have been recently presented at ESMO 2021 and confirmed the efficacy of the combination. Women receiving ribociclib plus letrozole had a median OS of 63.9 months compared to 51.4 months in the placebo arm (HR 0.76, p =0.004), with a 6-year survival rate of 44.2% versus 32%. ORRs were 42.5% with ribociclib versus 28.7% with placebo (p <0.0001) in the overall population and 52.7% versus 37.1% among patients with measurable disease.
The MONALEESA-3 trial evaluated ribociclib plus fulvestrant or placebo plus fulvestrant in 726 post-menopausal advanced breast cancer patients who had received a previous endocrine therapy. The primary endpoint was PFS, while the secondary endpoints included OS and ORR. Progression-free survival was improved by 7.7 months with ribociclib (median PFS 20.5 months) compared to placebo (median PFS 12.8 months), with a statistically significant HR of 0.59 (p <0.001). In a subsequent descriptive analysis, the median PFS increased to 33.6 months in the experimental arm with a 19.2 months value in the control group. OS was also significantly extended with ribociclib (Not Reached [NR] vs 40.0 months with placebo; HR 0.72, p = 0.005) and this result was confirmed by a recent update (median OS 53.7 months with ribociclib vs 41.5 months with placebo, HR 0.73). Objective responses were achieved by 32.4% of all patients treated with ribociclib and 21.5% of those receiving placebo, while among subjects with measurable disease ORR was 40.9% in the experimental arm and 28.7% in the control arm.
Finally, the MONALEESA-7 study specifically evaluated ribociclib plus endocrine therapy (i.e., letrozole or tamoxifen plus a luteinizing hormone releasing hormone analog) in 672 pre- and peri-menopausal women with advanced breast cancer. Patients could have received a previous chemotherapy but not endocrine therapy in the advanced setting. In this trial, PFS was the primary endpoint whereas OS and ORR were secondary endpoints. Median PFS was 10.8 months longer with ribociclib compared to placebo (23.8 months vs 13.0 months; HR 0.55, p <0.0001). In the pre-specified interim analysis, median OS was not reached in the experimental arm and 40.9 months in the control arm (HR 0.71, p =0.01), whereas an updated analysis after longer follow-up showed a median OS of 58.7 months with ribociclib vs 48.0 months with placebo (HR 0.76). The rate of objective responses was significantly higher with ribociclib than with placebo both in the total population (41 versus 30%) and in the population with measurable disease (51% versus 36%).
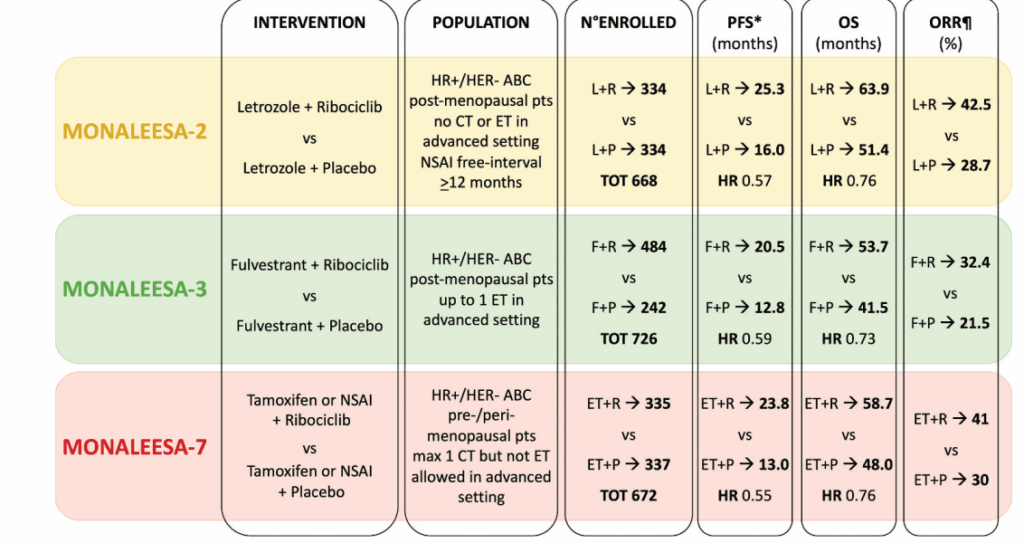
Figure 1. Overview of the MONALEESA Trials *PFS was the primary endpoint in all trials; ORR in the total population. Legend: CT chemotherapy; ET endocrine therapy; F fulvestrant; HR hazard ratio; HR+ hormone receptor-positive; HER2- human epidermal growth factor receptor 2 negative; L letrozole; N number; NSAI nonsteroidal aromatase inhibitor; ORR objective response rate; OS overall survival; P placebo; PFS progression-free survival; R ribociclib.
2.2 Efficacy Outcomes in Specific Populations
Several subgroup analyses, either pre-specified or not, demonstrate ribociclib efficacy in HR+/HER2- advanced breast cancer. Results from selected populations of the MONALEESA trials are detailed below and summarized in Table 1.
2.2.1 Age
In the MONALEESA-2 trial, ribociclib plus letrozole determined a comparable benefit between women younger than 65 years (n =373, of which 184 in the experimental arm and 189 in the control arm) and those aged ≥65 years (n =295, of which 150 in the experimental arm and 145 in the control arm). Hazard ratio for PFS was 0.52 among younger patients (median PFS NR in the experimental arm vs 13.0 months in the control arm) and 0.61 in the older ones (median PFS NR in the experimental arm vs 18.4 months in the control arm), without a significant interaction between the two age groups (p =0.6). At the time of the analysis, OS data were not mature in both populations, while response rates were numerically higher with ribociclib than placebo, regardless of age.
Age subgroups – <65 vs ≥65 years – were also evaluated in the MONALEESA-3 trial. In this study, 387 patients belonged to the younger group (258 in the experimental arm and 129 in the control arm) and 339 to the older one (226 in the experimental arm and 113 in the control arm). Age did not influence the efficacy of ribociclib plus fulvestrant over placebo plus fulvestrant in terms of PFS (HR 0.60 in both subgroups) and OS (HR 0.73 <65 years and 0.72 ≥65 years).
Among the MONALEESA-7 trial patients, 186 were aged <40 (98 in the experimental arm and 88 in the control arm), while 486 were ≥40 years old (237 in the experimental arm and 249 in the control arm). The addition of ribociclib to endocrine therapy reduced the risk of disease progression by 56% in patients <40 years and by 41% in those ≥40 years. In a recent analysis, OS was also improved by ribociclib in both groups, but the benefit was greater in women younger than 40 (median OS 51.3 months in the experimental arm vs 40.5 months in the control arm; HR 0.65) than in older ones (median OS 58.8 months in the experimental arm vs 51.7 months in the control arm; HR 0.81).
2.2.2 Site of Metastases
Visceral metastases, particularly those localized in the liver, confer an inferior prognosis compared with bone-only disease in HR+ breast cancer patients. In all MONALEESA studies, the presence of liver or lung metastases represented a stratification factor.
In the MONALEESA-2 trial, 373 (56%) patients presented metastases in the liver or the lung. At the second interim analysis, the benefit of ribociclib plus letrozole in terms of PFS was maintained in this population, with a 44% risk reduction of progression or death compared with placebo plus letrozole, versus 41% in patients without liver/lung metastases.
Similarly, in the MONALEESA-3 trial, 363 (50%) patients displayed liver or lung metastases. In the primary analysis, this subgroup showed an HR for PFS of 0.65, versus 0.56 in patients without lung/liver disease. Updated OS results demonstrated a superimposable benefit of ribociclib plus fulvestrant in the two groups, with an HR of 0.73 in patients with and 0.74 in those without liver/lung disease. Another analysis of the MONALEESA-3 trial specifically focused on the OS of patients with hepatic disease, showing a substantial benefit of ribociclib plus fulvestrant in this population (median OS 36.1 months in the experimental arm vs 24.1 month in the control arm).
In the MONALEESA-7 study, the number of patients with liver or lung metastases was 343 (51%). For these women, the risk of progression or death was halved by the addition of ribociclib to endocrine therapy, while it was reduced by 36% in patients without liver or lung metastases. In terms of OS, no difference emerged in the two subgroups, with an HR of 0.73 in the presence of liver/lung metastases and 0.70 in their absence.
2.2.3 De Novo Metastatic Disease
Up to 6% of breast cancers patients display metastatic disease at the time of diagnosis, with at least half of them presenting HR+ disease.
In the MONALEESA-2 trial, PFS evaluation among de novo metastatic women represented a pre-specified exploratory analysis. Thirty-four percent (n =227) of the enrolled subjects had primary metastatic disease, and they were equally distributed between the experimental and the control arm. In this population, median PFS was not reached with ribociclib plus letrozole with a 16.4 months value in the placebo plus letrozole population (HR 0.45), with an estimated PFS rate at 12 months of 82% in the experimental arm versus 66% in the control arm.
A lower percentage of patients (19%, n =139) presented with de novo metastatic disease in the MONALEESA-3 trial – i.e., 20% in the experimental arm and 17.4% in the control arm – but the outcomes of these subgroups have not been reported.
The MONALEESA-7 trial included the highest rate of de novo metastatic women, which represented 40% of the total population (270 patients), balanced between the experimental and the control arms. According to the subgroup analysis, ribociclib benefit in terms of PFS was particularly relevant in this subset of patients, with an HR of 0.43. OS data in this subpopulation are not yet available.
2.2.4 Endocrine Resistance
The development of resistance among breast cancer patients receiving endocrine therapy is an unavoidable event. Endocrine resistance can be primary – when disease relapses within 24 months in the (neo-)adjuvant setting or progresses within 6 months in the metastatic setting – or secondary – when the tumor relapses after 24 months of (neo-)adjuvant therapy or progresses after 6 months of therapy for advanced disease. The onset of primary resistance is predictive of an inferior outcome, and effective treatments are urgently needed for this population.
In the MONALEESA-3 study, 78 patients (11%) developed primary resistance during (neo-)adjuvant treatment or first-line therapy for metastatic disease. Median PFS among these patients was 13.4 months in the ribociclib plus fulvestrant arm versus 5.7 months in the placebo plus fulvestrant arm (HR 0.62). A 5.8 month OS advantage was obtained with the addition of ribociclib to fulvestrant in this population (median OS 37.5 months vs 31.7, HR 0.7).
In the MONALEESA-7 trial, 85 patients (13%) displayed primary endocrine resistance, as they progressed during the first 24 months of hormonal (neo-)adjuvant therapy. Nevertheless, ribociclib improved the outcomes of this patient population, as the median PFS was 14.5 months with ribociclib and 5.6 months with placebo (HR 0.56), while the median OS was not reached in the experimental arm and 32.7 in the placebo arm (HR 0.59).
2.2.5 Intrinsic Subtypes
HR+/HER2- breast cancer displays great heterogeneity in terms of genomic features. Indeed, gene expression profiles through the PAM50 gene signature can change the classification of up to 38% of the luminal A-like and 50% of the luminal B-like tumors.
In a retrospective analysis, 1160 tumor samples from patients enrolled in the three MONALEESA trials (672 in the experimental arms and 488 in the control arms) underwent genomic profiling with PAM50. Intrinsic subtypes were distributed as follows: 542 (46.7%) luminal A, 278 (24.0%) luminal B, 163 (14.0%) normal-like, 147 (12.7%) HER2-enriched and 30 (2.6%) basal like. In the luminal A group, the median PFS was 29.6 months in the ribociclib arm versus 19.4 months in the placebo arm (HR 0.63, p 0.0007), while in the luminal B group it was 22.2 versus 12.8 months (HR 0.52, p < 0.0001). Among normal-like tumors, median PFS was doubled with ribociclib (22.4 months versus 11.1; HR 0.47, p <0.001) and it was three-fold longer in the experimental arm in HER2-enriched cancers (16.39 months versus 5.52 months; HR 0.39, p <0.0001). Finally, PFS did not differ between the two arms in basal-like tumors (3.71 months versus 3.58 months; HR 1.15, p 0.77). Hence, all tumor subtypes derived a significant PFS improvement by the addition of ribociclib to endocrine therapy, with the exception of basal-like disease.
2.2.6 Dose Reduction
Dose reductions represent an effective strategy to manage the most common adverse events of ribociclib, but their impact on drug efficacy remains controversial. To this end, a pooled analysis of the MONALEESA-2, −3, and −7 studies correlated ribociclib dose reductions with outcomes. Only subjects receiving first-line therapy with an aromatase inhibitor or fulvestrant were included in this analysis for a total of 1066 patients in the experimental arms and 823 in the control arms. Women receiving tamoxifen in the MONALEESA-7 trial were excluded since the combination of ribociclib and tamoxifen is not indicated in the clinical practice. Among patients on ribociclib, 46% underwent a dose reduction, mainly due to neutropenia. Outcomes were evaluated according to relative-dose intensity, namely ≤71%, 72–96%, or ≥97%. Progression-free survival exhibited minimal differences between the three subgroups (24.8 months in the ≤71% group, 24.9 months in the 72–96% group, and 29.6 months in the ≥97% group). Similarly, ORR and clinical benefit rates were only slightly inferior in patients with lower dose intensity. Hence, dose reduction does not significantly affect ribociclib efficacy.
3. QUALITY OF LIFE AND PATIENT-REPORTED OUTCOMES
3.1 Quality of Life: Measurement Tools
According to the World Health Organization, QoL is ‘an individuals’ perception of themselves, of their position in life, in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns’. Health-related QoL (HR-QoL) is part of this broader concept and is referred only to factors which influence a subjects health. Since QoL and HR-QoL are strictly subjective, data concerning these parameters must be directly reported by patients in order to be translated in the so-called patient-reported outcomes (PROs). To this end, specific measurement tools are needed, such as validated questionnaires.
The EuroQol five dimensional – three levels (EQ-5D-3L) is a descriptive questionnaire recording five different aspects of HR-QoL (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) on three different levels (no problems, moderate problems, and extreme problems), which has been later implemented into the EQ-5D-5 levels (EQ-5D-5L) (i.e., five possible answers for each dimension). Despite not specifically addressing cancer patients, these questionnaires have been broadly used in the field of oncology.
On the contrary, the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30 (EORTC QLQ-C30) has been developed to register cancer patient PROs. Its 30 items allow to evaluate five functional scales (physical, role, emotional, cognitive, and social), eight symptoms (fatigue, pain, nausea/vomiting, dyspnea, insomnia, appetite loss, constipation, and diarrhea), financial difficulties, and global health status (GHS). The QLQ-C30 can be further integrated by a breast cancer-specific questionnaire (EORTC QLQ-BR23), which encompasses 23 items on systemic therapy side effects, concerns about hair loss, body image, future perspectives, sexuality.
Pain represents one of the main QoL determinants among cancer patients and specific tools exist for the self-assessment of this symptom. The brief pain inventory (BPI) represents a validated questionnaire, largely employed for the evaluation of cancer-related pain, especially in its short form (BPI-sf). It comprises nine items, including one question about the pain of the day, a diagram for pain localization, four questions about pain intensity, two about medications, one regarding pain interference with different aspects of everyday life.
3.2 Patient Reported Outcomes
Patient-reported outcomes were included in all the MONALEESA trials, using different questionnaires (Figure 2).
In the MONALEESA-2 study, patients were asked to complete EORTC QLQ-C30 and EORTC QLQ-BR23 at baseline, every two cycles for the first 18 months, every three cycles thereafter and at the end of treatment. Questionnaire completion rates were ≥75% throughout treatment in both arms, ranging from 98.5% on cycle 7, day 1 in the placebo arm 75.0% on cycle 25, and day 1 in the experimental arm. Global Health Status (GHS)/QoL scores were similar in the experimental and in the control group at baseline and in the subsequent evaluations, as well as time to definitive deterioration (TTD) (i.e., a ≥ 10% decrease in GHS score compared to baseline, with no subsequent increase), with an HR of 0.94. Symptom scores (fatigue, nausea, vomiting, and diarrhea) were low at baseline and slightly increased during the treatment among patients receiving ribociclib. However, these changes remained below the established significance threshold and did not affect the overall QoL. Similar results were registered for functional scores (physical, emotional, cognitive, ad social), which were high at baseline and underwent minimal decreases in the ribociclib arm. However, pain scores were meaningfully improved (>5 points) from week 8 to week 15 of treatment among patients receiving ribociclib. This result was confirmed by an exploratory analysis of the area under the curve (AUC) which evaluated changes in pain scores during therapy. Overall, GHS and pain worsened after the treatment discontinuation, especially in patients experiencing disease progression.
The EQ-5D-5L, EORTC QLQ-C3C30, and BPI-sf were employed in the MONALEESA-3 trial, at the same timepoints used for the MONALEESA-2. During the first year of treatment, the adherence rate for questionnaire completion was high (≥80%) in both arms, but at cycle 22 it dropped to 43% in the experimental arm and 41% in the placebo arm among first-line patients and to 27% in the experimental arm and 16% in the placebo arm among ≥2 line patients. Quality of life scores were superimposable between experimental and control groups with an improvement during the treatment period and a decline after therapy discontinuation in both arms. Time to definitive HR-QoL deterioration ≥10% was numerically longer in the ribociclib arm compared to placebo (35.9 months versus 33.1 months; HR 0.81). Symptom scores were similar between the two arms and did not vary significantly during treatment, while functioning scales showed a trend in favor of ribociclib in terms of TTD ≥10%. Additionally, patients receiving ribociclib seemed to attain better results in terms of pain control, especially when this symptom was assessed using the BPI-sf. Again, the occurrence of progression markedly influenced QoL, with scores deteriorating at the end of treatment and better outcomes among patients devoid of disease progression.
In the MONALEESA-7 study, PROs were assessed using EORTC QLQ-C30, EORTC QLQ-BR23, EBR23, and Q-5D-5L on day one of each cycle. Compliance rate was high, with 90% of patients in the experimental arm and 83% in the control arm completing questionnaires at baseline and at least at another timepoint. Modifications in GHS were similar among patients receiving ribociclib and those receiving placebo, but TTD≥ 10% was significantly delayed by the addition of ribociclib to endocrine therapy (35.8 months in the experimental arm versus 23.3 months in the control arm; HR 0.67). The ribociclib arm was superior in terms of fatigue, physical, social, emotional functioning. Similarly, pain was improved and better controlled among patients receiving ribociclib (HR for TTD ≥10% in pain scores 0.67). As observed in the MONALEESA-2 and −3 trials, patients without a PFS event had longer TTD ≥ 10% (median not reached) compared to patients with disease progression (median 24 months) with a 0.31 HR.
A pooled QoL analysis has been conducted taking into account all patients enrolled in MONALEESA-2, women treated with first-line endocrine therapy in MONALEESA-3 and patients treated with an aromatase inhibitor in MONALEESA-7, for a total of 1528 subjects. In line with the findings of the individual studies, GHS scores were maintained during treatment in the two arms, while time to definitive deterioration ≥10% favored ribociclib (39.6 months in the experimental group and 33.1 in the placebo group; HR 0.79). Ribociclib determined a delay in TTD ≥ 10% in GHS regardless of patient age, race, and intrinsic breast cancer variant. Emotional functioning favored ribociclib as well, while a less pronounced benefit was observed for fatigue, physical and social functioning. In this pooled analysis, pain scores improved in both arms from baseline to cycle 3 and TTD ≥ 10% in pain was not reached in both arms although the benefit was greater with ribociclib (HR 0.71). As expected, GHS and pain scores worsened at the end of treatment both in the experimental and the control group.
4. CONCLUSION
To our knowledge, no work has focused on reviewing the results of ribociclib subgroup analyses and patient-reported outcomes thus far. Here, we summarized data about ribociclib activity across different subpopulations of the MONALEESA trials, demonstrating a strikingly consistent benefit even for patients with an inferior prognosis. Additionally, our review of PROs from the MONALEESA studies confirms that QoL is preserved among patients receiving ribociclib plus endocrine therapy, regardless of the treatment setting. Given these results, the combination of ribociclib plus endocrine therapy represents a mainstay for the treatment of advanced HR+/HER2-breast cancer patients. In the forthcoming future, results from ongoing studies will likely define unresolved questions, such as the impact of molecular selection of patients (SOLTI-1201 HARMONIA trial) or the role of ribociclib in the adjuvant setting (NATALEE trial).
5. EXPERT OPINION
The combination of a CDK4/6 inhibitor with endocrine therapy is currently the standard of care for the first-line treatment of advanced HR+/HER2-breast cancer. The success of this class of drugs relies on their efficacy, combined with an acceptable toxicity spectrum which minimally impacts patient QoL.
PD-0332991, ribociclib, and abemaciclib share a common molecular target, but they display distinct pharmacokinetic/pharmacodynamic features, along with different results in phase III trials. Presently, ribociclib is the only CDK4/6 inhibitor with a consistently significant OS advantage in the first line setting for both pre- (MONALEESA-7) and post-menopausal (MONALEESA-2) breast cancer patients but also in the second-line setting (MONALEESA-3). Of note, the final median OS registered in the experimental arm of the MONALEESA-2 study (63.9 months) is the longest ever reported in a phase III trial enrolling advanced breast cancer patients. Additionally, ribociclib plus fulvestrant determined a greater numerical gain in terms of OS in the MONALEESA-3 trial (12.2 months) compared to abemaciclib plus fulvestrant in the MONARCH-2 trial (9.4 months) and to PD-0332991 plus fulvestrant in the PALOMA-3 trial (6.9 months). However, a direct comparison between these studies is not appropriate, since the MONALEESA-3 and MONARCH-2 trials enrolled patients with up to one prior endocrine treatment and no chemotherapy lines in the metastatic setting, while the PALOMA-3 study also included heavily pretreated patients with several previous endocrine therapy and/or chemotherapy lines.
Results from the analysis of ribociclib efficacy according to the intrinsic subtypes showed that the combination of CDK4/6 inhibitors with endocrine therapy retains its efficacy in patients with HER2-enriched and normal-like disease, while these drugs fail to exert a meaningful effect on basal-like tumors. This observation has fuelled an increasing interest toward translational studies which include molecular profiling of breast cancer. For example, the phase III SOLTI-1201 HARMONIA trial will enroll HER2-enriched HR+/HER2-advanced breast cancer patients to receive ribociclib or PD-0332991 plus endocrine therapy. This trial will be the first to directly compare two CDK4/6 inhibitors while also selecting patients according to the intrinsic subtype of their disease.
Moving from the advanced to the early-phase setting, the ongoing phase III NATALEE (NCT03701334) trial is testing ribociclib and letrozole as adjuvant therapy for breast cancer patients with locally advanced non-metastatic disease. Results from this study are eagerly awaited and will shed light on the potential role of ribociclib in early breast cancer.
Patient-reported outcomes are available from all phase III trials featuring CDK4/6 inhibitors, but again cross-trial comparisons should be interpreted cautiously as different measurement tools and methodologies have been used across these studies. Overall, CDK4/6 inhibitors do not negatively affect patient QoL and GHS, while all three molecules share a trend toward pain improvement. Still, the proportion of patients experiencing a decline in QoL while on treatment has not been reported. This represents an important missing data for a thorough interpretation of QoL results. The clear evidence emerging from PRO assessment in all CDK4/6 inhibitor trials is the tight bond between traditional ‘physician reported’ outcomes (i.e., PFS and OS) and patient-reported outcomes, as confirmed by a recent report, which shows that longer OS correlates better QoL in the MONALEESA-3 and −7 trials.
In conclusion, ribociclib is an excellent example of the successful strategy currently being pursued for the treatment of advanced breast cancer: balancing outstanding treatment efficacy for all affected women with meaningful improvements in their QoL. In the five years, additional findings from ongoing trials will determine if these benefits will also be amenable for women diagnosed with early breast cancer. Moreover, trials with a strong translational rationale, such as the HARMONIA study, will likely elicit the incorporation of breast cancer molecular profiling into clinical practice.